.png)
How can Vodder's MLD resolve trigger points without pain?
- Jan Douglass PhD

- Aug 20, 2019
- 6 min read
Updated: Feb 7, 2025
People are often surprised when I start talking about #MLD* to resolve trigger points, or treat conditions like #adhesive_capsulitis and #piriformis_syndrome. I'll leave piriforimis syndrome for another blog, but let's have a look at how the Vodder method of MLD* resolves #trigger_points, #joint_stiffness and #myofascial_pain. And why this is more effective than other forms of #triggerpointtherapy such as dry needling.

First question? What are trigger points?
There are many texts and online sources on the etiology and pathogenesis of trigger points, so there are many and varied descriptions of what is happening in the muscle and fascia. Commonly noted are the presence of inflammatory mediators in the fascia, an initiating event such as trauma or strain in the muscle, and stiffness or contracture of the fascia itself sometimes described as fibres 'sticking' together. Direct palpation is painful.
I haven't read all the available literature but the more I do read, the more I notice that no one is talking about the thixotropic properties of fascia and how this may contribute to trigger point formation (you can read my blog on thixotropy in the loose connective tissue here). All connective tissues in the body are thixotropic which means they can fluctuate between the sol and gel states (ie be more fluid like or more gel like).

The large glycosaminoglycan molecule hyaluronic acid imparts this property to the connective tissue. It is a long polysaccharide strand with a 'brush border' of binding sites for water molecules. Hyaluronic acid (also known as hyaluronan) binds most of the water in the interstitium but this can fluctuate to allow more free water (the sol state) or less free water (the gel state) to circulate. The enzyme hyaluronidase is responsible for moderating this fluctuation. When hyaluronidase levels are high hyaluronan releases water molecules to the interstitium. When hyaluronidase subsides the hyaluronan gathers up free water molecules again. Synovial fluid and fascia are thixotropic. In the synovial fluid hyaluronic acid allows the fluid to shift along the viscosity spectrum between the gel and sol states according to the need for protection against compression forces (the gel state) or friction damage (the sol state). In the fascia of muscles, tendons and ligaments hyaluronan regulates fascial gliding. When most of the water is held in the hyaluronan molecules fascial gliding is restricted and may be felt as 'stiffness'. When water molecules are released as free water fascial gliding is facilitated.

You may have noticed hyaluronic acid promoted in beauty products where it is used topically to hold water in the epidermis to reduce the appearance fine lines, and also as an injectable (Wikipedia).
Hyaluronans also have essential roles in tissue organisation and cell proliferation (see ref 1 below).
All tissue cells can manufacture hyaluronan and it plays an important role in inflammation by helping to recruit inflammatory cells and cytokines and regulating the expression of inflammatory genes. It can attenuate the course of inflammation to protect against tissue damage but hyaluronan deposits are also implicated in rheumatoid arthritis, lung disease, inflammatory liver disease, vascular disease, rejected kidney transplants and diabetic nephropathy, inflammatory bowel disease and colitis (see ref 1 below).
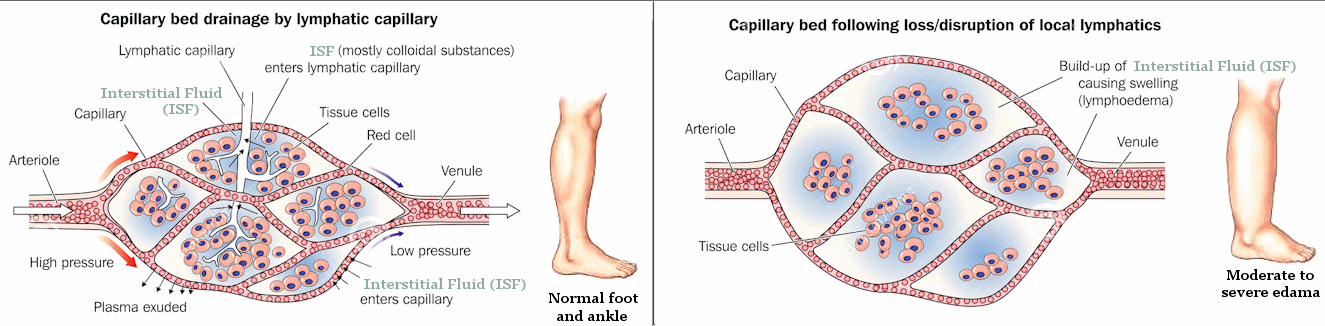
Inflammation also induces micro-oedema in the extracellular matrix via increased vascular filtration. These pockets of fluid increase the distance between tissue cells and their supplying capillary, slowing down diffusion of essential molecules such as the respiratory gasses. If these micro oedemas persist, cell hypoxia follows and can lead to impaired organ function.
Next question, what does this have to do with trigger points? Everything!
All the descriptions of trigger points that I read talked about the presence of inflammation and 'stiffness' or 'stickiness' in the fascia. Some sources related this to the build if of cellular wastes at the trigger point location, or previous trauma to the muscle.

The traditional way to deal with this in physical therapy has been to apply sustained compression forces into the trigger point to forcibly release the fascia. More recently dry needling has become very popular and a Google Scholar search reveals a large number of systematic reviews on dry needling. None found strong evidence for dry needling for trigger points other than short to medium term pain relief. None found long term benefits beyond 12 weeks or any significant functional improvement or improved quality of life (ref 2 - 4 are just the 3 top results).
Why will MLD work better?
Most people will recognise MLD* as a light, pain free movement of the skin and subcutaneous tissue which creates shearing forces in the tissue and increases lymph motorcity. The gentle but repetitive shearing forces applied to the tissues raises the level of hyaluronidase and a more fluid state of the tissue is achieved. Simultaneously the increased rate and amplitude of lymphatic pumping increases suction on the affected tissues and trapped macromolecules and excess fluid is drawn out of the interstitial spaces. Inflammatory cycles are interrupted and normal tissue architecture returns.

These techniques may also be used to palpate more deeply into fascia, tendons, ligaments and direct muscle attachments. Progressively deeper palpitations are used and the client guides the identification of small pockets of inflammation. Once located, lighter, pain free techniques are used to drain the tissue. This test - treat - retest protocol is very precise and allows for the precise and effective treatment of isolated pockets of inflammation such as at trigger points. Once the inflammatory mediators are removed and facial gliding is restored the 'trigger point' disappears. Since this method of treating only requires brief palpation to locate the inflammatory deposits and all treatment is applied pain free, the whole experience for the client is pleasant and relaxing. More importantly, and in contrast to painful compression techniques or needling, the results can be permanent. If the therapist is thorough and takes the time to locate and drain even the smallest inflammatory deposits, chronic inflammatory processes are interrupted, normal tissue function is restored and many cases of chronic pain resolve completely without relapse.

I wish I could list numerous systematic reviews on the use of MLD* to release trigger points, but unfortunately there are no studies on this topic - we're always too focussed on measuring the effects of MLD in lymphoedema management!
There are a couple of good reports on MLD for fibromyalgia which demonstrate the effect of MLD in restoring fascial functioning. A RCT in 2009 comparing massage therapy and MLD showed positive effects in both groups but the benefits in the group receiving MLD were significantly greater than the massage group (ref 5). A cohort study published in 2003 reported that pain, stiffness, sleep, sleepiness, and well-being all improved during MLD treatment. Benefits (other than sleep) were still significantly improved two months after the treatments had finished, and after a further 3 months (5 months total) significant improvement remained in pain and sleepiness (ref 6).
Within the next few months we will announce a new Certificate in Applied MLD - essentially the current Therapy 1 techniques with more application to pathologies. This course will offer a Vodder MLD qualification to therapists who want to treat sporting injuries, chronic pain and release trigger points all without pain, but who may not want to learn lymphoedema management. It will also allow therapists with an existing lymphoedema qualification the opportunity to safely resolve skeletal muscular issues for clients who may otherwise unsuitable to receive deep remedial techniques. To ensure you are notified of this new certificate as soon as it is available, subscribe to the MLD Newsletter here. You will also find all previous newsletters on that page.
* All references to MLD in this article refer only to Dr Vodder's MLD as taught by Instructors accredited by the Vodder Akademie International, Walchsee Austria.
References
Petrey, A.C. and C.A. de la Motte, Hyaluronan, a crucial regulator of inflammation. Frontiers in immunology, 2014. 5: p. 101-101.
Liu, L., et al., Effectiveness of dry needling for myofascial trigger points associated with neck and shoulder pain: a systematic review and meta-analysis. Archives of physical medicine and rehabilitation, 2015. 96(5): p. 944-955.
Morihisa, R., et al., Dry needling in subjects with muscular trigger points in the lower quarter: a systematic review. International journal of sports physical therapy, 2016. 11(1): p. 1.
Cagnie, B., et al., Evidence for the use of ischemic compression and dry needling in the management of trigger points of the upper trapezius in patients with neck pain: a systematic review. American journal of physical medicine & rehabilitation, 2015. 94(7): p. 573-583.
Ekici, G., et al., Comparison of manual lymph drainage therapy and connective tissue massage in women with fibromyalgia: a randomized controlled trial. Journal of Manipulative and Physiological Therapeutics, 2009. 32(2): p. 127-133.
Asplund, R., Manual lymph drainage therapy using light massage for fibromyalgia sufferers: a pilot study. Journal of Orthopaedic Nursing, 2003. 7(4): p. 192-196.



Comments